U.S. immigration raids in Minnesota drive patients to underground care

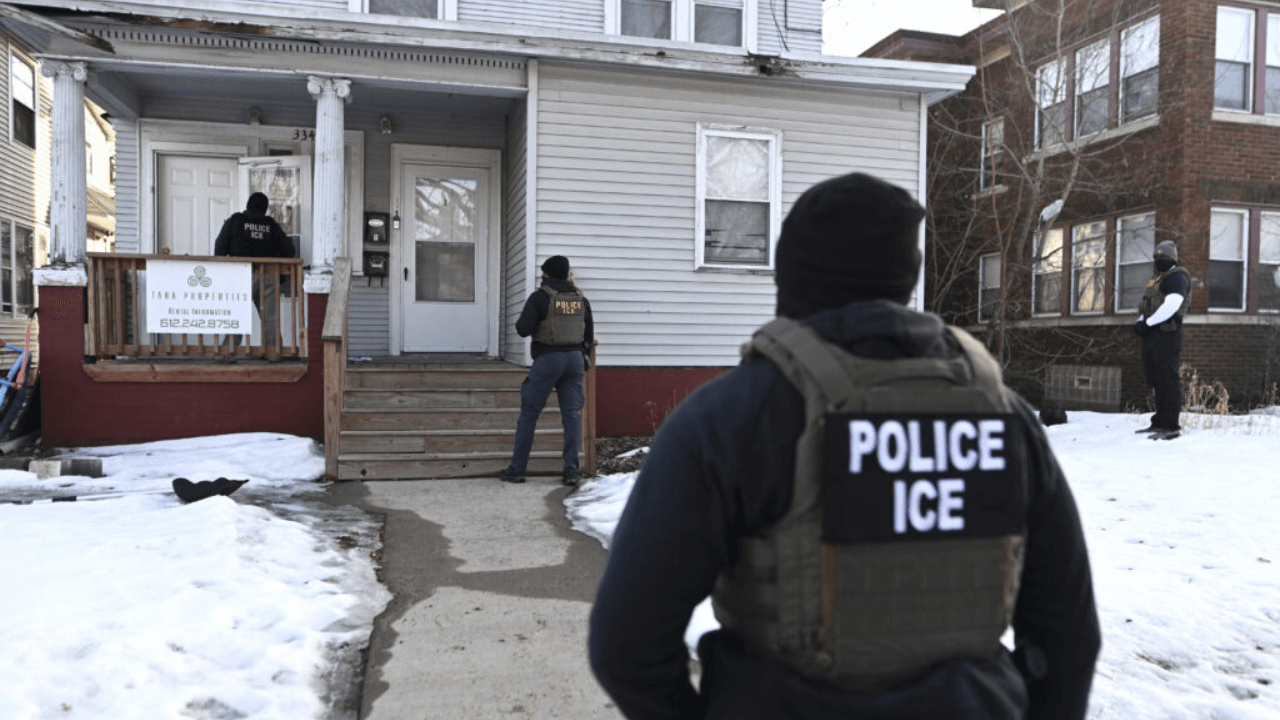
MINNEAPOLIS, MINNESOTA — United States Immigration and Customs Enforcement (ICE) raids in Minnesota have pushed many immigrant families to avoid hospitals and clinics, forcing health workers to quietly organize informal home-based care networks as appointment cancellations and no-show rates surge across local health systems.
According to a report from MinnPost, the human toll is reflected in the story of Gabi, a 2-year-old U.S.-born child with a rare genetic condition that makes her bones brittle. Her surgery, which doctors hoped would help her walk someday, was canceled after her family feared leaving home during federal immigration operations.
“I want more than anything for my baby to walk,” her mother said in Spanish. “But with the situation that’s happening, I canceled the surgery and all the physical therapy appointments… Because I’m afraid to leave.”
How U.S. immigration crackdowns impact medical care
Healthcare providers across Minnesota say the situation has had measurable operational consequences. Some medical systems have reported appointment cancellations and no-show rates reaching 60% since December, leaving clinicians struggling to reach vulnerable patients who now avoid hospitals.
At the same time, doctors, nurses, and community volunteers have quietly begun providing care outside traditional medical settings.
“I used to look somebody in the eyes and say, with good faith, ‘You will be fine at the hospital,’” said Emily Carroll, a nurse practitioner at HealthFinders Collaborative in Faribault. “But now, I can’t make that guarantee.”
As immigration enforcement operations became more aggressive, healthcare workers reported that some agents established posts at hospital parking areas, which made it more difficult for patients who already feared arrest or deportation to access medical care.
Building shadow healthcare networks for vulnerable patients
To solve this problem, health workers are building informal care networks that provide care at homes and around community spaces. These parallel systems rely on volunteer coordination, discreet outreach, and trusted local contacts to connect patients with medications, follow-ups, and basic clinical services.
Minnesota Democratic state Senator Alice Mann, a physician, said the experience offers a warning for other communities facing similar pressures.
“I know it sounds crazy,” she said, but healthcare providers “need to start an underground network of how to get people care in their homes. Because letting people die at home or come close to death because they are terrified to go into the hospital, in 2026, is outrageous.”
What Minnesota’s crisis means for global health systems
For hospitals and healthcare operators, the Minnesota experience highlights how facility-centric care models can quickly break down when communities feel unsafe accessing traditional care settings.
The disruption shows the need to build a system that provides distributed and remote-first medical services that can continue to operate during times of social and political unrest.
Health systems now use centralized telehealth systems with multilingual nurse helplines and contracted patient support services to connect with patients who need care outside medical facilities. The models enable healthcare providers to keep track of their high-risk patients while they manage their treatment needs and operational activities.
Health systems could also design an “above-ground” version of Minnesota’s informal care networks through structured programs such as offshore nurse triage lines, centralized telehealth hubs, outsourced patient outreach teams, and social determinants of health (SDOH) logistics support.
Providers can use digital care operations with analytics that track no-shows, missed treatments, and high-risk patients to discover care gaps that they can resolve before patients leave their treatment.
For healthcare leaders, Minnesota’s experience serves as both a warning and a blueprint: when trust in physical healthcare spaces erodes, resilient systems must be able to reach patients wherever they are.






